WHAT DO YOU NEED?
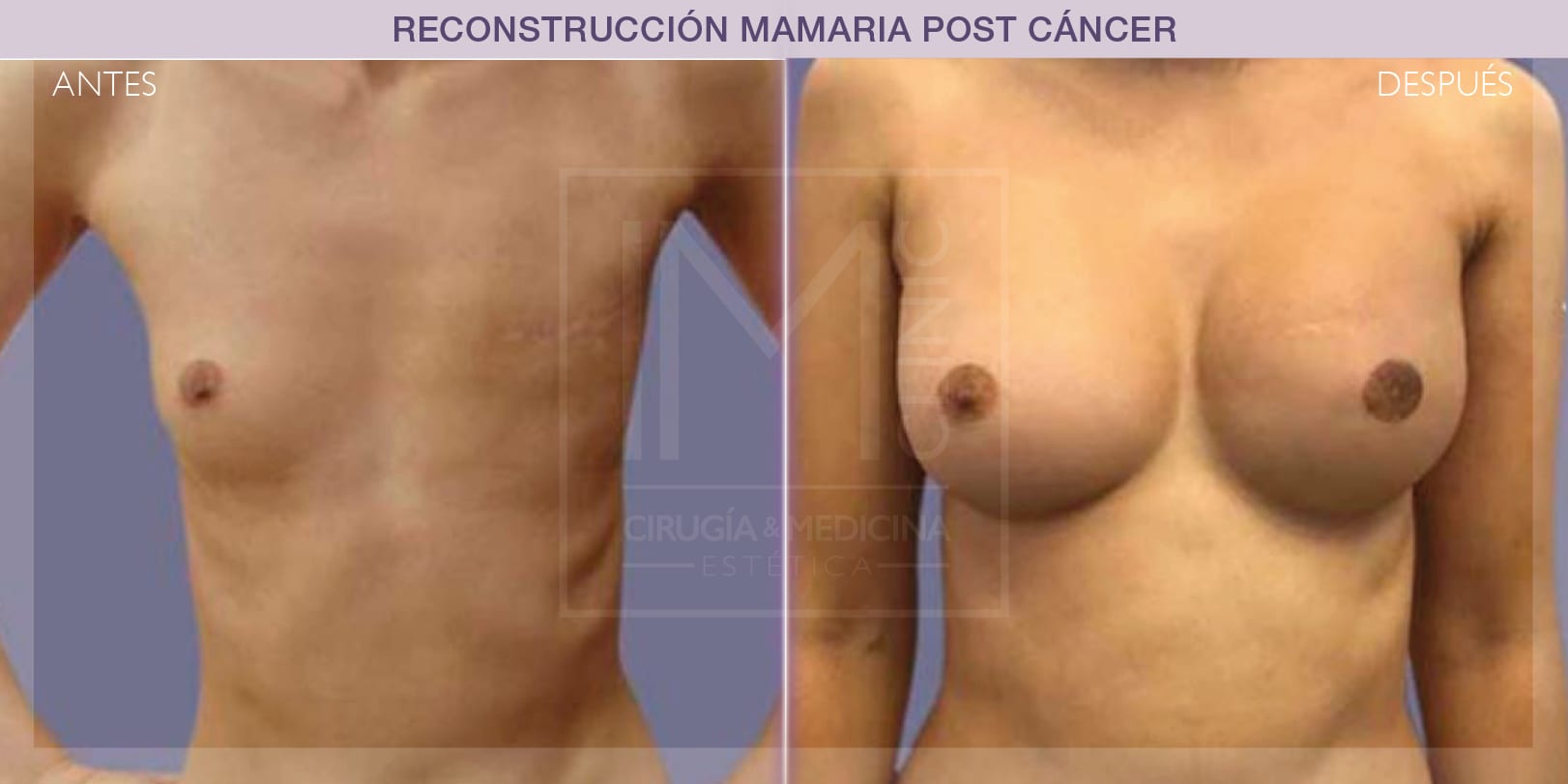
Breast reconstruction with expander
Breast reconstruction with expander consists of inserting an empty implant that is gradually filled with saline solution until it is the right size and can be replaced with an implant. In this case, the areola and nipple are also reconstructed.

Breast reconstruction with enhancement of both breasts
Many women deciding to undergo breast reconstruction also decide to enhance the other breast. This provides extremely satisfactory results. The areola and the nipple are also reconstructed in this case.





Who can have breast reconstruction surgery?
Any patient who has had a mastectomy or any woman who is to have full or partial breast removal might be a candidate for breast reconstruction.
Breast reconstruction with expander
This technique can only be selected when the surgeon performing the mastectomy was able to save all the skin covering the breast. This breast reconstruction can be performed during mastectomy surgery or some time later.
This post-mastectomy breast reconstruction technique consists of inserting a temporary inflatable breast implant under the pectoral muscle (breast region). To make the skin and/or muscle distend, the implant is gradually filled with saline solution in outpatients. This means that, after a few months and thanks to the elastic properties of the skin, the tissues are distended far enough to remove the expander and replace it with a final breast implant. There are, however, expanders that do not require removal.
As the expander is being inflated, the patient can undergo the radiotherapy or chemotherapy treatments prescribed by the doctor without this having any impact on the breast reconstruction or on the disease.
Later on, the nipple and areola are reconstructed, if necessary. The end result is a breast that is very similar to the other, allowing the woman to recover her body identity and forget the injuries caused by the disease.
After breast reconstruction surgery with expander, the patient can return to everyday life within three to five weeks.
Flap breast reconstruction
Flap breast reconstruction consists of using tissue from near the breast area (known as “flaps”). This second technique is more complicated than the first, as part of the operation requires microsurgery to mobilise the skin, fat, muscle and vascular structure of another part of the body (back, abdomen). This means that its recovery period is also longer.
Candidates for this breast reconstruction technique include mastectomised patients not considering the option of breast implants, either by personal decision or because it is not advised, particularly in cases where the patient must be subject or has been subject to radiotherapy treatment.
Of the different options available, the technique of choice currently considered is DIEAP. In this surgery, skin and fat are taken from the abdomen along with an artery and a vein for irrigation, are removed from the body and are then transplanted into the same patient in the breast area to be reconstructed. The skin, fat and vessels are removed without damaging the muscles of the abdominal wall (avoiding hernias, eventrations, bulges and weaknesses of the abdominal wall), and this surgery is also less painful than traditional techniques.
The advantage of DIEAP flap breast reconstruction is that it allows for complete reconstruction using the patient’s own tissue; skin tissue and fat that will behave much more naturally, both physically and biologically, than that obtained from implant reconstruction. Another major benefit is the abdomen enhancement, giving the patient a svelte figure and firm abdomen after surgery.
Breast reconstruction with fat grafting
This technique is based on replacing the volume of the breast by grafting the patient’s own fat. This is autologous fat obtained using liposuction that is rich in growth factors and that also helps improve the tissue quality.
Candidates for this breast reconstruction technique are those who have had conservative surgery without removal of the entire breast. It is also used as a concomitant method in patients who have received radiotherapy. The presence of growth factors among the fat cells allows for regeneration of the tissue damaged by radiation.
The surgery consists of liposuction in which enough fat is removed to reconstruct the breast. This fat is washed, processed and treated before being inserted into the area to be reconstructed using small cannula. The volume of fat that can be injected is not unlimited and depends on the characteristics of the tissue, the quality of the fat obtained, and the characteristics of the patient (smokers, for example, tolerate less volume). Several sessions are therefore normally required to obtain the desired volume. This means that a smaller amount of fat is injected in each session, thus maximising the survival rate of the grafted cells.
The duration of the surgery varies, and depends on the amount of fat to be obtained, its processing time, and the need for any parallel procedure. On average, it takes around 2-3 hours. It is generally performed under general anaesthesia. However, in cases where it is only required to remodel some isolated aspect of the breast, it can be performed under local anaesthesia with sedation.
Hospitalisation time also varies, with one overnight stay at IM CLINIC being the most frequent.
Fat grafting, either as a primary reconstruction technique or as a adjuvant technique, offers excellent results in terms of restoring the appearance of the breast and recovery of the tissue quality
After surgery, the patient must be particularly careful with impact to or pressure on the grafted area. A girdle must be worn for four weeks in the area where the liposuction was performed. You can return to everyday life 72 hours after surgery, and you can go back to work in 7-10 days and resume sporting activities after one month.
Areola reconstruction
While surgical breast reconstruction is possible, reconstruction of the areola can be performed surgically or using a dermopigmentation technique.
The surgical technique for areola reconstruction consists of reconstructing an areola with the same shape and size as the other areola. A skin graft is performed in the inguinal or labia minora area to reconstruct the texture and pigmentation of the areola. Local flaps are normally used for the nipple. This is an outpatient procedure that can be performed under local anaesthesia. The results are definitive, although there might be certain depigmentation of the areolar graft over time.
The dermopigmentation technique consists of injecting mineral pigments into the surface of the skin using microneedles. The skill and expertise of the therapist will create an appearance that is the same as the patient’s original areola. Dermopigmentation provides a very realistic reproduction, although without any texture. Because the pigments are located very near the surface of the skin, they progressively lose shape and the procedure must be repeated every 3-5 years.
In both cases, the results are extremely satisfactory and almost reproduce a real areola. The combination of both procedures is commonplace for optimum results.
POSTOPERATIVE CARE: AFTER BREAST RECONSTRUCTION SURGERY
You can return to a normal diet after surgery. However, try to eat smaller meals more often for the first few days until your rhythm of digestion has returned to normal.
You must sleep on your front for at least the first month after your breast reconstruction surgery. This, however, will depend on the recovery of each individual patient.
You will be wearing a special bra after breast augmentation surgery, which you must wear with a band during the first month after surgery. This will depend on your recovery.
Make sure the incisions are properly dry after your shower. We advise applying cold air (never hot!) from a hair dryer. Do not rub a towel over the incisions.
If you smoke, you should try to stop before your breast augmentation surgery. This will improve your health and your healing capacity.
Could breast reconstruction make the cancer come back?
Not at all. Breast reconstruction has no impact on the evolution of the disease. Although many women are ‘afraid’ about further surgery in the area, there are many studies to show that there is no relationship between the evolution of the disease and the different post-mastectomy breast reconstruction techniques.
When is the best time to have breast reconstruction surgery?
It would be ideal to be able to plan the surgery for breast reconstruction at the same time as the mastectomy because the tissues are of a better quality than later on once they have healed.
However, the results when performed during later surgery are also extremely good.
Can breast reconstruction surgery be performed even though it has been a long time since the mastectomy?
Yes, the only problem is that you must undergo another surgery. It is, however, more advisable to have the surgery at the same time as the mastectomy, especially for psychological reasons.
Can it have an impact on the treatments of the disease?
In these cases, the surgery has no impact on the evolution or the treatment of the disease. The oncologists and plastic surgeons must communicate to ensure the overall treatment of the disease.
Does breast cancer exist in men?
Of course, although to a lesser extent than in women. Only one in every one hundred cases are in men. Both the prognosis and the treatment are the same as for women, although it is normally detected at a later stage in men because, given its infrequency, other diagnoses are often suggested beforehand.
Can I have mammograms after breast reconstruction surgery?
Yes, if the doctor recommends it. It is important to make sure you find an imaging centre that specialises in this type of examinations on women who have undergone breast reconstruction surgery and inform of this circumstance before you have a mammogram.
Is it possible to improve the appearance of both breasts?
At IM CLINIC we advise our patients to improve the appearance of the other breast to ensure an attractive, balanced end result.
In some cases, the patient decides to remove glandular tissue from the healthy breast to prevent cancer from appearing in that breast.